SARS-2 CoV
CDC is misleading the public by reporting the per 100,000 rate instead of the actual percentages
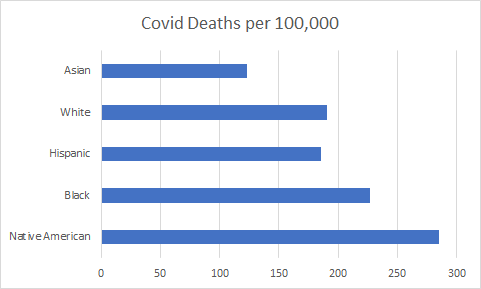
CDC is misleading the public by reporting “per 100,000” rather than actual numbers. The chart above makes it look like the Native American population is being ravaged by Covid-19, but is misleading due to small percent of total population.
Per 100,000 is a rate, not an actual number. It is only good for comparing within a fixed population/ group, not between different sized populations/groups. This applies to different racial/ethnic groups, age groups, states, counties. The smaller the total population, the larger the “per 100,000” appears. If a population is 10 and only 1 is affected, that is 10,000 per 100,000. If the population is 1000 and 1 is affected, that is 100 per 100,000. The technique magnifies results in smaller populations and reduces results in larger populations.
Example: January, 2021 data from USAfacts.org reported deaths per 100,000 by ethnic group. Each group has a different size and percent of total population. Deaths per 100,000 is reported so that Native Americans appear to be the most affected by far because the population is relatively small. See table below.
| Ethnic Group | Group Population | Group as Percent of US Pop. | Covid Deaths per 100,000 | Number of Covid Deaths | Covid Deaths as percent of total deaths |
| Native American | 6,371,200 | 2 | 285.1 | 18,164 | 3.0 |
| Black | 40,138,560 | 12.6 | 227.1 | 91,154 | 15 |
| Hispanic | 53,836,640 | 16.9 | 185.7 | 99,975 | 16.5 |
| White | 197,507,200 | 62 | 190.8 | 376,843 | 62 |
| Asian | 16,565,120 | 5.2 | 123 | 20,375 | 3.4 |
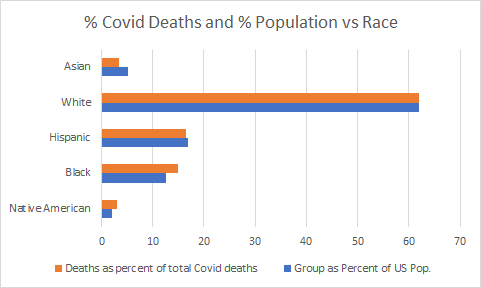
By converting the per 100,000 results reported into actual numbers and percentage of the total deaths, the picture is quite different and similar to the percent of US population for each group. The huge disparity has disappeared. Blacks and Native Americans appear to be slightly more affected, while Hispanics and Asian are slightly less affected than their population.
Epidemiology to take seriously: Natural immunity better than COVID vaccines — JunkScience.com
Epidemiology to take seriously: Natural immunity better than COVID vaccines — JunkScience.com
A new epidemiology study reports that natural immunity confers better protection against COVID than current vaccines. I’ve been publishing JunkScience.com for 25+ years and can’t think of a single epidemiology study I’ve seen that was worth anything. 31 more words
Original scientific paper from research team in Israel is attached.
Israeli Study Conclusive: Natural Immunity Better Than Vaccinations
Media Hype about “Long Covid”

Science Norway reports Poor studies on long Covid are sensationalized by the media Excerpts in italics with my bolds.
Many recent reports in the media have given the impression that people are experiencing major long-term effects after having even mild Covid-19. This impression does not correspond with the knowledge we have accumulated so far.
We must dedramatise the long-term effects of Covid-19, often referred to as long Covid. The media have a responsibility in this regard. They must become more critical of the research methods used in the studies they refer to.
Most infectious diseases with severe symptoms will to some extent be accompanied by long-term effects. Most infectious diseases with mild symptoms will cause few short-term effects.
More and more studies are showing that this is probably also the case for Covid-19. It is vital that more high-quality studies are carried out to examine this problem.
Data…
View original post 379 more words
CDC dropping RT-PCR test for Covid-19
CDC is ending RT-PCR testing in favor of multiplex rapid antigen test to distinguish Covid from Flu. See CDC notice below. What they are not telling us is that the RT-PCR test has very high false positives, inflating the numbers. The rapid antigen test is more accurate and gives results in minutes, so medical care decisions can be made ASAP. Labs will start transitioning before the Dec 31, 2021 cutoff so numbers will start to drop, just in time for 2022 election year. England has been using the rapid antigen test for over a year.
07/21/2021: Lab Alert: Changes to CDC RT-PCR for SARS-CoV-2 Testing

Audience: Individuals Performing COVID-19 Testing
Level: Laboratory Alert
After December 31, 2021, CDC will withdraw the request to the U.S. Food and Drug Administration (FDA) for Emergency Use Authorization (EUA) of the CDC 2019-Novel Coronavirus (2019-nCoV) Real-Time RT-PCR Diagnostic Panel, the assay first introduced in February 2020 for detection of SARS-CoV-2 only. CDC is providing this advance notice for clinical laboratories to have adequate time to select and implement one of the many FDA-authorized alternatives.
Visit the FDA website for a list of authorized COVID-19 diagnostic methods. For a summary of the performance of FDA-authorized molecular methods with an FDA reference panel, visit this page.
In preparation for this change, CDC recommends clinical laboratories and testing sites that have been using the CDC 2019-nCoV RT-PCR assay select and begin their transition to another FDA-authorized COVID-19 test. CDC encourages laboratories to consider adoption of a multiplexed method that can facilitate detection and differentiation of SARS-CoV-2 and influenza viruses. Such assays can facilitate continued testing for both influenza and SARS-CoV-2 and can save both time and resources as we head into influenza season. Laboratories and testing sites should validate and verify their selected assay within their facility before beginning clinical testing.
Opt in to receive updates from the CDC Laboratory Outreach Communication System (LOCS).
Online resources:
- FAQ: CDC Distribution of COVID-19 Assays
- Guidance for SARS-CoV-2 Point-of-Care Testing
- Interim Guidance for SARS-CoV-2 Antigen Testing
- Interim Guidelines for Collecting, Handling, and Testing Clinical Specimens for COVID-19
- Frequently Asked Questions about COVID-19 for Laboratories
- Information for Laboratories about COVID-19
- CDC COVID-19 Website
- Clinical Laboratory COVID-19 Response Weekly Calls
- CDC Laboratory Outreach Communication System (LOCS)
If you have any questions, please contact us at LOCS@cdc.gov.
Thank you,
The Laboratory Outreach Communication System
Laboratory Outreach Communication System (LOCS) | Division of Laboratory Systems (DLS)
Center for Surveillance, Epidemiology, and Laboratory Services (CSELS)
Centers for Disease Control and Prevention (CDC)
Covid-19 tests have high false positives
The article below from Epoch Times reveals the problem that inflates Covid-19 case numbers. PCR tests are great diagnostic tests for confirming the source of an illness; PCR is a terrible screening test for non-symtomatic people. You may also read the original article using the link at the end.

World Health Organization (WHO) Director-General Tedros Adhanom Ghebreyesus gives a press conference at Geneva’s WHO headquarters on Feb. 24, 2020. (Fabrice Coffrini/AFP via Getty Images)PUBLIC HEALTH INFORMATION
WHO Changes CCP Virus Test Criteria in Attempt to Reduce False Positives
BY MEILING LEE January 23, 2021 Updated: January 24, 2021
The World Health Organization (WHO) has cautioned experts not to rely solely on the results of a PCR test to detect the CCP virus.
In updated guidance published on Jan. 20, the WHO said that lab experts and health care practitioners should also consider the patient’s history and epidemiological risk factors alongside the PCR test in diagnosing the CCP (Chinese Communist Party) virus.
The new guidance could result in significantly fewer daily cases.
“Most PCR assays are indicated as an aid for diagnosis, therefore, health care providers must consider any result in combination with timing of sampling, specimen type, assay specifics, clinical observations, patient history, confirmed status of any contacts, and epidemiological information,” the guidance says.
It’s unclear why the health agency waited over a year to release the new directive. The WHO didn’t reply to an inquiry from The Epoch Times.
Scientists and physicians have raised concerns for many months of an over-reliance on and a misuse of the PCR test as a diagnostic tool since it can’t differentiate between a live infectious virus from an inactivated virus fragment that is not infectious.
Additionally, the high cycle threshold values of most PCR tests—at 40 cycles or higher—increases the risk of false positives. A higher threshold value indicates less viral load and that the person is less likely to be infectious, while a person with a lower cycle threshold value has a higher viral load, or is more infectious.
The WHO did not specify what the threshold value cutoff should be for a positive diagnosis, but said to only “determine if [a] manual adjustment of the PCR positivity threshold is recommended by the manufacturer.”

However, it clarified that when the prevalence of the CCP virus is low, “the risk of false positive increases” meaning that “the probability that a person who has a positive result (SARS-CoV-2 detected) is truly infected with SARS-CoV-2 decreases as prevalence decreases, irrespective of the claimed specificity [of the PCR test].”
SARS-CoV-2 is the scientific name for the CCP virus that causes the disease COVID-19.
The Centers for Disease Control and Prevention (CDC) says its PCR tests have a cycle threshold cutoff of 40 cycles. The federal agency finally included information on cycle threshold value in its Frequently Asked Questions about COVID-19 for laboratories on Nov. 12, 2020.
But many medical experts consider a threshold value cutoff of 40 cycles to only return false positives since samples that go through many amplification cycles will pick up negligible RNA sequences regardless if the virus is inactivate or the viral load is exceedingly low to pose any problem.
Prior to the CCP virus pandemic, for individuals to be considered a case, they must test positive and show clinical signs and symptoms. But to be counted as a CCP virus case, only a positive PCR test is required. And no matter how many times an individual is tested, each positive test is counted as a separate case.
The WHO is now advising that a positive PCR test that does “not correspond with the clinical presentation” should be verified by taking “a new specimen” and retesting it.
This advice may also help lower CCP virus cases in hospitals as it more clearly defines who is considered a hospitalized case.
The UK’s National Health Service (NHS) Director of International Relations Dr. Layla McCay confirmed to talkRADIO that a percentage of hospitalized patients officially counted as positive cases were actually being treated for different illnesses not related to COVID-19. They had only tested positive for the disease at the hospital without displaying any symptoms.https://platform.twitter.com/embed/index.html?creatorScreenName=EpochTimes&dnt=false&embedId=twitter-widget-0&frame=false&hideCard=false&hideThread=false&id=1346363750006317056&lang=en&origin=https%3A%2F%2Fwww.theepochtimes.com%2Fwho-changes-ccp-virus-test-criteria-in-attempt-to-reduce-false-positives_3668064.html&siteScreenName=EpochTimes&theme=light&widgetsVersion=ed20a2b%3A1601588405575&width=550px
Dr Layla McCay, NHS Confederation director, confirms to Julia that the hospital figures for “Covid patients” include patients who are not being treated for Covid but have simply tested positive while being treated for something else.@JuliaHB1 | @LaylaMcCay pic.twitter.com/xSud6LW13M
— talkRADIO (@talkRADIO) January 5, 2021
“It is correct that in hospital, people who tested positive for COVID will be the full range of symptoms,” McCay said. “Some will have it as an aside to some other problem for which they’re in the hospital.”
The day after the WHO released its new guidance, Chief Medical Adviser to President Joe Biden, Dr. Anthony Fauci, said the United States would rejoin the organization.
“As such, I am honored to announce that the United States will remain a member of the World Health Organization,” Fauci said. “Yesterday, President Biden signed letters retracting the previous administration’s announcement to withdraw from the organization, and those letters have been transmitted to the secretary-general of the United Nations and to you Dr. Tedros, my dear friend.”
Tedros Adhanom Ghebreyesus is the director-general of the WHO.
“The United States also intends to fulfill its financial obligations to the organizations,” Fauci added.
In July last year, the Trump administration pulled out of the WHO over its alleged role in helping the Chinese communist regime cover up the severity of the CCP virus.
There have been mixed responses from Congress over Biden’s decision to rejoin the WHO.
Rep. Lauren Boebert (R-Colo.) introduced a bill (pdf) on Jan. 21 to “prohibit the availability of United States contributions to the World Health Organization until Congress receives a full report on China and the COVID-19 pandemic, and for other purposes.”
She said in a statement: “The WHO is China-centric and panders to Beijing at every turn. There is no reason U.S. taxpayers should contribute more than $400 million annually to an organization that covered for China and failed to contain the spread of the COVID-19 pandemic.”
Prior to former President Donald Trump withdrawing from the WHO, the United States contributed the most money to the health agency, according to State Department statistics.
What Really Happened? — Candidly Speaking

Bulletin Of Atomic Scientists Opens The Wuhan Virus Pandora’s Box BY TYLER DURDENWEDNESDAY, MAY 05, 2021 – 10:10 PM Authored by Nicholas Wade via the Bulletin of the Atomic Scientists (emphasis ours), The COVID-19 pandemic has disrupted lives the world over for more than a year. Its death toll will soon reach three million people. Yet […]
What Really Happened? — Candidly Speaking
I recommend this article for those who want a true and complete picture of the origin of the Covid-19 virus. References are reliable and comprehensive. – Kay Kiser, author of Perverted Truth Exposed
Investigation into origins of Covid-19, part 2
Click on the link above to view video of Part 2 of Steve Hilton’s investigation into the origins of Covid-19.
Investigation into origins of Covid-19, part 1
Click on the link above to view video of Steve Hilton’s investigation into the origins of the Covid-19 virus.
