Are most cases of HIV/AIDS in Africa really misdiagnosed endemic diseases?
Are most cases of HIV/AIDS in Africa really misdiagnosed endemic diseases?
The Claims: HIV/AIDS from unsafe heterosexual contact is rampant in Africa. Many children are left as orphans because both parents have died from AIDS.
The Truth: While HIV/AIDS is undoubtedly present in Africa and other destitute areas, there are problems with its reported transmission, diagnosis and treatment. HIV infections in the developed world occurs almost exclusively among homosexual males and IV drug users who share needles with infected people, and heterosexual transmission is rare. In Africa, half of those diagnosed with HIV and HIV/AIDS are heterosexual women, so there must be other mitigating circumstances. It is possible that actual infections are acquired through non-sterile injections in contraceptive clinics. This could help to explain why HIV in Africa is diagnosed equally among men and heterosexual women. It is very likely that HIV and HIV/AIDS are over diagnosed in Africa and other poverty stricken areas of the world with or without actual HIV testing. Many cases of AIDS in Africa may have little or no connection to the HIV virus or indiscriminate sexual practices. Those that are malnourished or have chronic diseases such as TB or malaria naturally have compromised immune systems, i.e. Acquired Immune Deficiency Syndrome, AIDS, from these conditions without carrying the actual Human Immunodeficiency Virus (HIV).
Because of poor healthcare facilities and abilities, HIV/AIDS may be diagnosed based on symptoms without HIV testing in many rural and isolated areas. In other areas, where actual testing for HIV antibodies is done, a high incidence of false positives is likely to occur. This is due to the poor specificity of the test and reaction with antibodies from other diseases and conditions. Most of those diagnosed with HIV/AIDS, whether tested or untested for HIV, have been assumed to have full blown HIV/AIDS through disparate symptoms recognized by the UN WHO including fever, headache, rash, sore throat, swollen lymph nodes, weight loss, chronic diarrhea or cough, all of which can be caused by many common parasites or infectious diseases as well as severe illnesses such as malaria and tuberculosis (TB). UN WHO has named TB as a leading indicator of HIV/AIDS and lists TB as causing 2/3 of HIV/AIDS deaths. HIV/AIDS itself does not cause death; it opens the way for other diseases that kill people. Reporting TB deaths as HIV/AIDS deaths without confirmation of HIV bolsters the statistics, as does reporting orphans as AIDS orphans. At this time it is impossible to know how prevalent over diagnosis is in Africa and other poor areas.
Over diagnosis of HIV and HIV/AIDS, when promoted by the international media, paints a picture of Africa that packs a triple whammy for AIDS advocates and international population control governmental and nongovernmental organizations. First, it excuses high death rates and failure to treat endemic diseases; secondly, it incentivizes HIV/AIDS research funding in developed countries by falsely declaring AIDS a heterosexual pandemic; thirdly it has the potential for vindicating population control programs in the minds of potential donors by creating a false picture of rampant immorality and promiscuity. As a bonus, it also encourages the use of condoms that furthers population control agendas.
HIV facts and questions:
HIV causes AIDS: Unlike those who deny that HIV causes AIDS or that it even exists, I do not deny that HIV causes AIDS or that HIV exists. I do question some of the current statistics, testing and treatment options. Because it is politically incorrect to question the UN WHO recommended practices and conclusions, those who question the status quo will undoubtedly be accused of denialism by AIDS advocates in order to conflate, confuse, discredit and silence anyone daring to question the efficacy of the current testing and treatment methods, even when it might lead to better understanding and improved protocols.
Non-HIV AIDS: TB, Malaria, dysentery and other serious chronic diseases cause a more common form of Acquired Immune Deficiency Syndrome, AIDS, that has no connection to HIV/AIDS or sexually indiscriminate behavior. It is well known that anyone who is chronically ill and/ or malnourished naturally has a compromised immune system. Other opportunistic diseases are easily acquired by persons whose immune systems are compromised. By labeling these non-HIV AIDS cases as HIV/AIDS, it can be an excuse for not treating the underlying conditions.
Unfortunately, for USAID, UN WHO and activist NGOs or agencies that provide aid to poor countries, because their emphasis is on required or coerced population control and not on treating disease, many clinics do not have the basic medicines, equipment or facilities to treat endemic diseases, but have store rooms filled with birth control drugs, condoms and other birth control and abortion materials and equipment. This is a human tragedy and a crime against humanity that must be stopped. It is unconscionable that Western aid not be heavily weighted toward supplying medicines and equipment for prevention and treatment of endemic diseases.
Recommendation: In both HIV/AIDS and non-HIV AIDS, treatment should always begin with addressing the presenting diseases and malnutrition. Once the patient is stabilized then HIV/AIDS treatment can begin, but only after further confirmation of the original diagnosis of HIV/AIDS. HIV/AIDS treatment drugs further compromise the immune system so that treatment of weakened, disease ravaged patients and those with non-HIV AIDS using these drugs may do more harm than good.
International aid organizations should be encouraged or required to reverse their decades old practice of oversupplying population control materials and under-supplying needed medicines, facilities, equipment and supplies to treat endemic diseases.
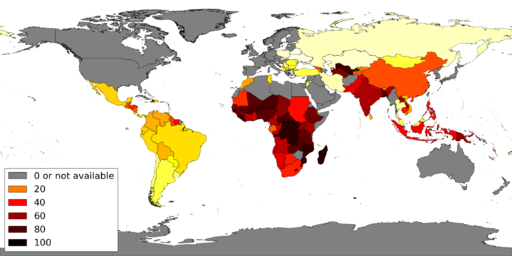
Demographic Shift: HIV/AIDS in developed countries is confined almost exclusively among homosexual men and IV drug users who share needles with HIV infected people. The expected pandemic in developed countries never materialized. According to official statistics, Sub-Saharan Africa accounts for 2/3 of the HIV incidence in the world, with Southern Africa, (South Africa and Botswana), accounting for most of that. 15 to 25% of the South African population has been diagnosed with HIV or HIV/AIDS. More than half of the HIV positive people in South Africa are heterosexual women. Heterosexual contact is blamed for causing the spread of HIV, but in other countries heterosexual transmission is very rare. Unless the HIV virus has mutated, this theory of frequent heterosexual transmission cannot be valid and other mitigating factors must be considered.
Shared needles as a possible source: One theory is that the reuse of hypodermic needles for injected birth control drugs is responsible for the spread of HIV, and, if true, could account for the higher incidence in women in Africa and other poor countries where injected birth control is required or advocated. Injectable birth control drugs such as Depo Provera that must be reinjected every 3 months are sometimes administered in a clinic, but more often the drug and the syringes are given to patients for administration at home. Because viruses do not live very long on surfaces outside the body, HIV could not be transferred unless an HIV infected person has used the needle just prior to reuse by a second person for birth control. This could only happen in a clinic where multiple women are injected one after another without proper sterilization of needles.
How are these in-home administered reused needles causing HIV/AIDS without an immediate HIV contamination source in each case? It is more likely that in-home injections with improperly sterilized needles would transfer opportunistic bacterial infections such as staph and strep. The whole idea of giving hypodermic syringes to uneducated people is ludicrous; it is the worst of the birth control methods, and the best way to spread more disease and misery. Poor women with little or no concept of microbial infective agents are unlikely to discard or destroy needles even if the package instructions say to discard after use.
Recommendation: If this form of birth control must be injected every 3 months, it should only be done by a professional in a clinic with properly sterilized or disposable needles. If birth control is desired, a better alternative would be insertion of an IUD, Intrauterine Device, which does not require regular follow up treatments.
Could Depo-Provera make women more susceptible to HIV infection? According to this theory, the active ingredient in Depo-Provera, (Depo-medroxyprogesterone acetate, aka DMPA), may chemically predispose at risk women to acquiring HIV through sexual contact with infected men, through thinning of vaginal epithelial cells and immunosuppression. Three recent meta-studies[1] show a statistically significant link between use of the drug and incidence of HIV in at risk women. The link to HIV transmission was not established statistically for use of either oral contraceptives or another injectable contraceptive drug, NET-EN, (norethisterone enanthate), in these studies.
Clinical Diagnosis without HIV testing: In rural poor areas of Africa HIV/AIDS may be diagnosed without HIV testing by the clinical indicators listed by WHO such as fever, headache, rash, sore throat, swollen lymph nodes, weight loss, chronic diarrhea or cough. These symptoms may also be caused by endemic diseases such as TB, malaria and other insect borne diseases, dysentery and other water borne diseases, parasites and malnutrition. WHO considers TB to be a leading indicator of HIV/AIDS. Some people diagnosed without HIV testing may instead have non-HIV AIDS caused by these endemic diseases.
Diagnosis with HIV testing: Clinical HIV tests detect antibodies to the virus, not the virus itself. HIV tests have a high incidence of false positives, so that retesting and other confirmation are needed after a positive test result. False positives of HIV testing may be the result of non-HIV AIDS caused by other diseases and pregnancy because the HIV tests are non-specific and may detect antibodies to other diseases or conditions.
Causes of False Positives: HIV testing is not specific to HIV and is prone to false positives. It tests for antibodies to HIV, not the virus itself, but can also detect other antibodies present in chronic diseases or those acquired over a lifetime. There are over 65 documented causes of false positives including TB, malaria, leprosy, hepatitis, Q fever, influenza or colds, herpes simplex, leishmaniosis, and Epstein Barr virus. Pregnancy or prior pregnancies are among factors that can cause false positives due to presence of HLA (human leukocyte antigen). Is it time to question whether HIV testing, without thorough validation, is valid in parts of Africa where the population is routinely exposed to numerous diseases that leave a heavy load of antibodies in their blood?
Validation needed for HIV positives: False positives are common so that, according to manufacturers’ instructions, positive tests must be retested in duplicate and then by another method to verify results, e.g. ELISA twice then Western Blot. ELISA, Enzyme Linked ImmunoSorbent Assay, uses an antigen for the (in this case HIV) antibody bound to a solid surface and an enzyme that causes a color change when the target antibody attaches itself to the antigen. Western Blot actually separates, by gel electrophoresis, each component in a mixture of antibodies bound to specific antigens. Medical testing protocols vary from country to country, so that the same test may be interpreted as positive or negative depending on the protocol. For example, UK does not use the Western Blot verification of duplicate ELISA tests, and different countries require from one to four Western Blot markers to verify and confirm a positive result.
South Africa uses duplicate ELISA only to verify positive HIV tests, resulting in 15-25% of the population testing positive, 60% of which are heterosexual women. South Africa also has a high rate of drug treatment for prevention of mother to child HIV transmission, which may mean that most HIV tests are conducted at gynecological clinics and obstetric hospitals on pregnant women. This is a problem since pregnancy is known to cause false positives. The incidence of HIV and AIDS in most of the other countries in Africa, and indeed the world, ranges from 0.1 to 5.0 percent of the population. South Africa’s 15 – 25% incidence needs a closer look. The fact that over half of these are heterosexual women is also problematic as described above.
Recommendation: South Africans and Botswanans when first diagnosed with HIV or HIV/AIDS need to be retested using a more stringent verification protocol in the future. Unfortunately, the drugs used for treating HIV can cause false negatives, so retesting those already receiving therapy may be useless or at lease confusing.
Opportunistic Diseases: When people sicken and die with HIV/AIDS, it is not the HIV that kills them; it is other opportunistic infections that are able to invade and thrive because HIV has crippled the immune system. TB is the leading cause of death in Africa, with or without HIV/AIDS. A diagnosis of HIV/AIDS can be an excuse not to treat underlying endemic diseases.
Treatment Options: HIV treatment drugs suppress the immune system further than the disease itself. Wouldn’t it make sense to treat the opportunistic diseases and malnutrition more aggressively first before suppressing the immune system further with AIDS treatment drugs? In some areas of Africa, TB and HIV are treated simultaneously, which is a step in the right direction.
Orphans from AIDS? AIDS orphans are defined as anyone 15 years or younger who has lost, depending on the country, their mother, one parent or both parents to “AIDS related diseases.” South Africa includes people up to 18 years old. WHO estimates that 70% of “AIDS orphans” have one living parent. TB is the leading cause of death in Africa and the leading clinical indicator of the presence of AIDS. Since many people in Africa live very short lives, with or without AIDS, how is this any different from the pattern of the past where lifespans are short and teenagers often are orphaned?
[1] References cited in Population Research Institute newsletter article: “While Admitting Risks, WHO Continues to Recommend Injectable Contraceptives for Women at High Risk of Contracting HIV” by Jonathan Abbamonte, April 20, 2017 as follows:
Brind J, Condly SJ, Mosher SW, Morse AR, Kimball J. Risk of HIV Infection in Depot-Medroxyprogesterone Acetate (DMPA) Users: A Systematic Review and Meta-analysis. Issues Law Med 2015; 30(2): 129-39.
Morrison CS, Chen PL, Kwok C, Baeten JM, Brown J, Crook AM, et al. Hormonal contraception and the risk of HIV acquisition: an individual participant data meta-analysis. PLoS Med 2015; 12(1): e1001778.
Ralph LJ, McCoy SI, Shiu K, Padian N. Hormonal contraceptive use and women’s risk of HIV acquisition: a meta-analysis of observational studies. Lancet Infect Dis. 2015; 15(2): 181-9.